
Collection:
Sinusitis
Rhinosinusitis is an inflammation of the respiratory mucosa affecting the nose, nasal cavities, and sinus ostia, whether or not accompanied by an infectious process.










CiliaCell Nasal Spray - Children
Choose your option

CiliaCell Nasal Spray - Adult
Choose your option

CiliaCell Nasal Spray - Adult SENSITIVE
Choose your option
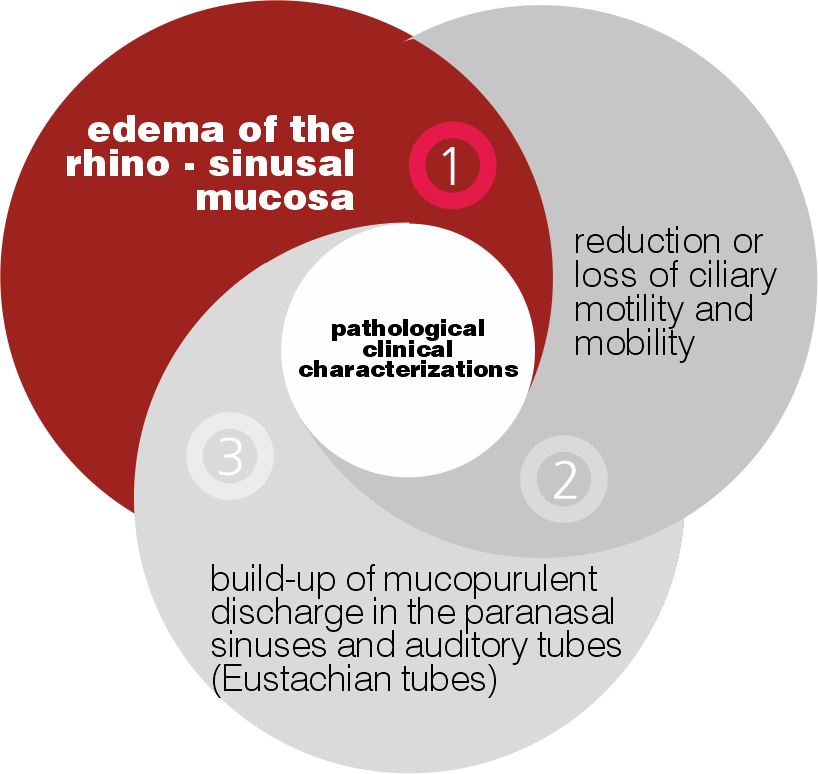
Clinical Characterizations of Sinusitis
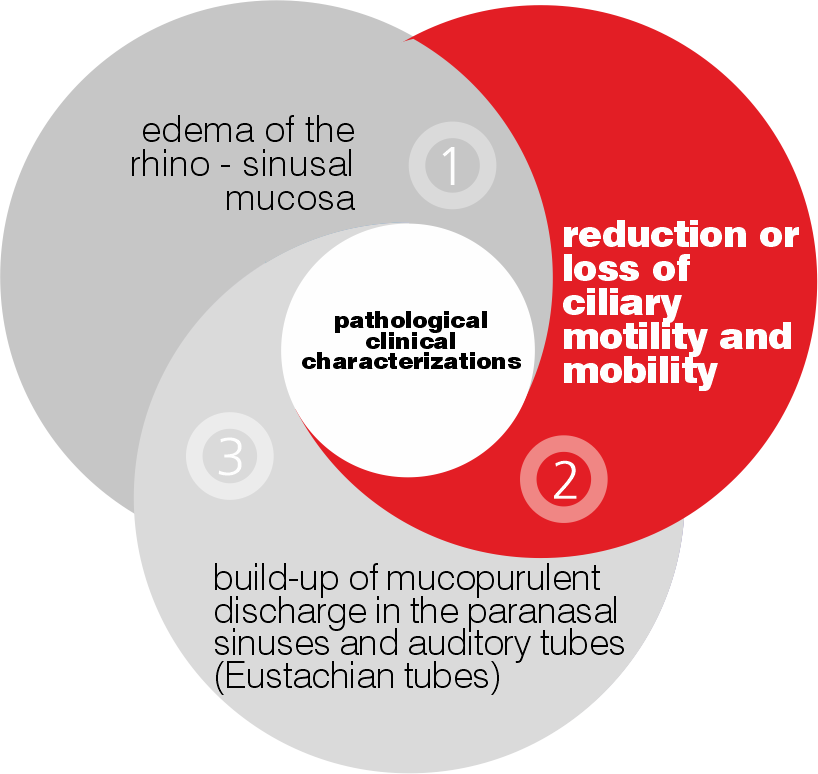
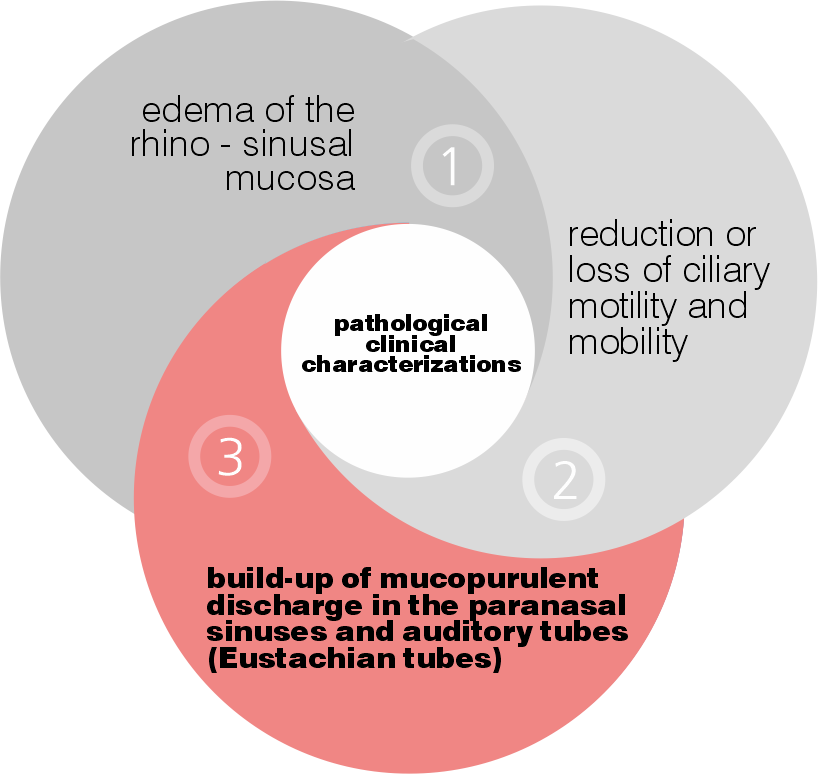
The most important clinical characterizations of rhinosinusitis are:
- Edema of the rhino-sinusal mucosa
- Reduction or loss of ciliary motility and mobility
- Build-up of mucopurulent discharge in the paranasal sinuses and auditory tubes (Eustachian tubes).
Rhino-sinus mucosal edema
Causes:
- Presence of infectious agents
- Phlogosis
Consequences:
- Partial or total occlusion of the com
- Alteration of pneumatization of the sinuses
- Mucus-pus accumulation in the rhino-sinus district
Reduction or blockage of ciliary mobility and motility
Causes:
- Phlogosis
- Mucus-pus accumulation in the rhino-sinus district
- Use of topical corticosteroids
Consequences:
- Persistence of mucus-pus in the rhino-sinusal district and proliferation of infectious agents
- Bacterial biofilm formation and evidence of phenomena of antibiotic resistance
Build-up of mucopurulent discharge in the paranasal sinuses and auditory tubes
Causes:
- Soft tissue edema
- Reduction of ciliary motility
- Presence of infectious agents
Consequences:
- Proliferation of infectious agents with possibile formation of biofilms
- Stopping ciliary mobility
- Chronicization of pathology
What are the symptoms of rhinosinusitis?
The symptoms of rhinosinusitis can vary depending on the etiology, that is, the factor or factors that caused it.
We can distinguish the following three types of rhinosinusitis:
SYMPTOMS
- Mucus discharge from the nose that is yellow or greenish in color, or you find it on the handkerchief when you blow your nose
- Facial pain in one or more places (above the jaws, around the eyes at the sides of the nose, at the forehead above the eyebrow arches, in the back of the skull)
- Sensation of not being able to smell
- Nosebleed
- Mucus going down the throat
- Symptoms in only one nostril of the nose (nasal obstruction, presence of purulent mucus, bleeding).
CAUSES
A very commonplace cold that lasts for more than 5-7 days, brought on by an infection caused by viruses, fungi, and/or pathogenic bacteria (Infectious rhinosinusitis).
SYMPTOMS
- Mucus discharge from the nose almost as clear as water, indistinctly from both nostrils
- Frequent sneezing even without the discharge of mucus from the nose
- Itchy nose
- Facial pain in one or more places (above the jaws, around the eyes at the sides of the nose, at the forehead above the eyebrow arches, in the back of the skull)
- Conjunctivitis with red or itchy eyes.
CAUSES
An underlying respiratory allergy, caused by exposure to particular types of allergens such as pollens, dust mites, chemicals…
SYMPTOMS
- Mucus discharge from the nose almost as clear as water, indistinctly from both nostrils
- Frequent sneezing even without the discharge of mucus from the nose
- Itchy nose
- Facial pain in one or more places (above the jaws, around the eyes at the sides of the nose, at the forehead above the eyebrow arches, in the back of the skull)
- Conjunctivitis with red or itchy eyes.
CAUSES
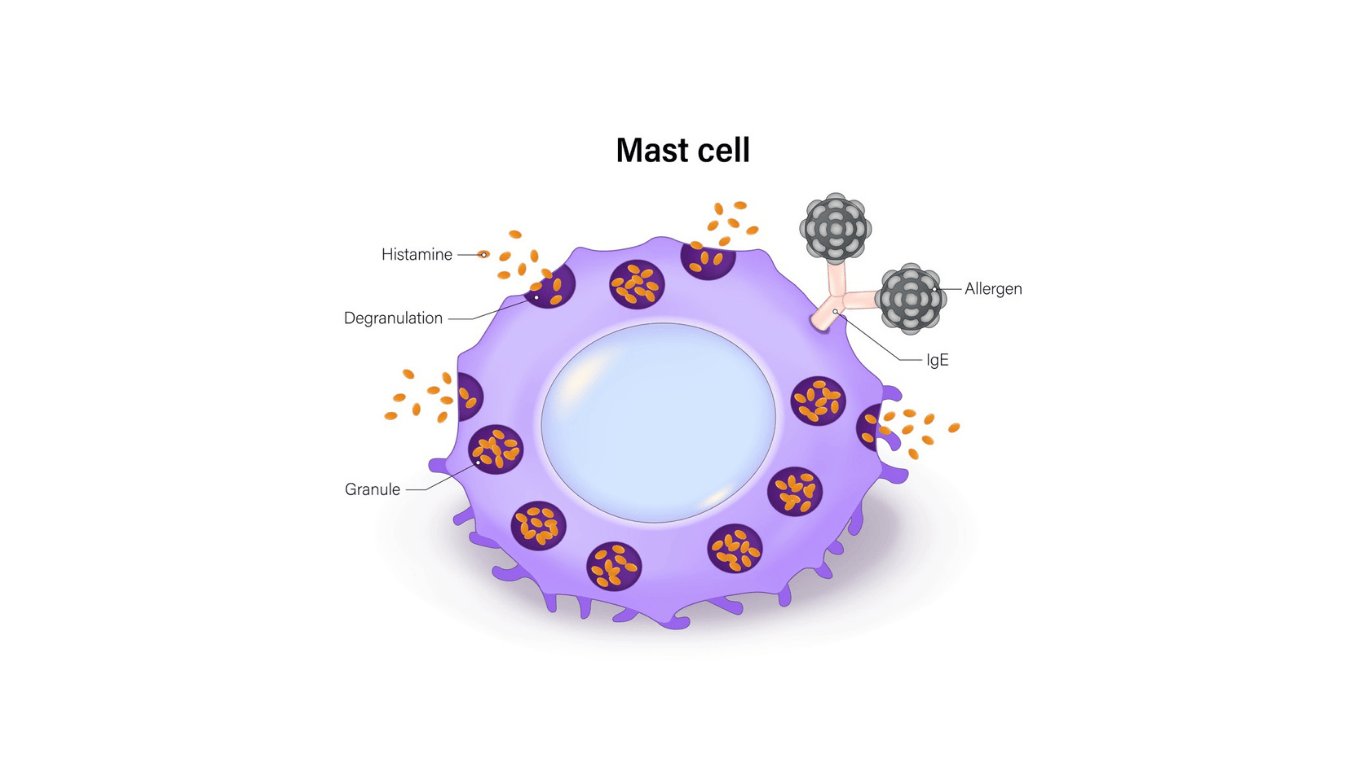
The presence of non-allergic cell-mediated rhinitis, caused by the dysfunction of certain cells found in the respiratory mucosa such as: mast cells, eosinophils and neutrophils). Depending on the cells affected by the dysfunction, the following cellular diseases are distinguished: nares, narne, narma, and naresma – nonallergic cell-mediated rhinosinusitis.
Photophobia, difficulty concentrating, and general malaise may also be present in all cases.
In case of infectious rhinosinusitis, the same symptoms may be accompanied by fever.
Why is pain felt in rhinosinusitis?
Regarding pain in rhinosinusitis, there is a myth to dispel, namely that pain results from inflammation of the respiratory mucosa. Actually, the pain that is felt is craniofacial pain, that is, neuropathic pain: in other words, pain resulting from inflammation (stimulation) of craniofacial nerves.
Basically what happens?
Basically what happens?
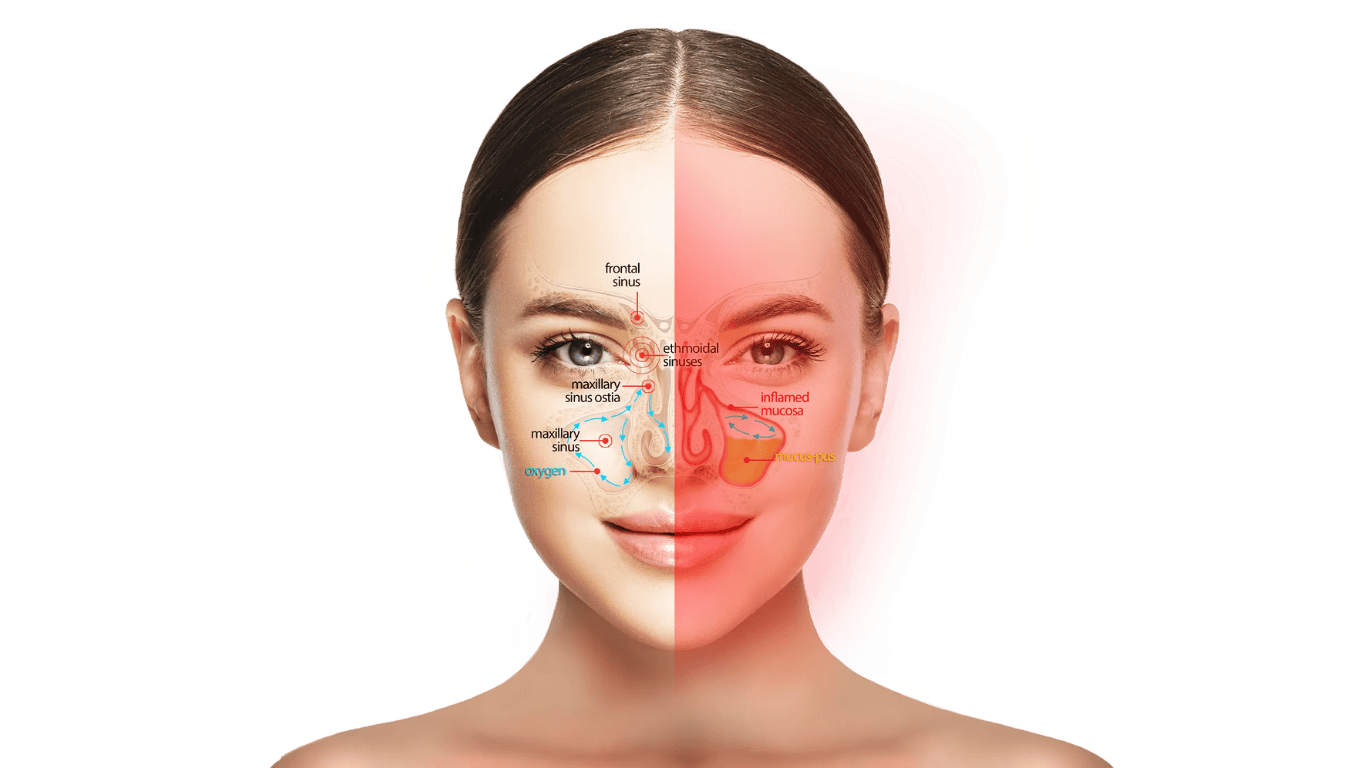
It is as simple as that! When the inflammation extends beyond the nasal cavities (about 5-7 days after what we can classify as a common cold), the same inflammation is also beginning to affect the mucosa lining the ostia of the paranasal sinuses (small 1-2 mm diameter ducts that connect the nasal passages to the paranasal sinuses). When it becomes inflamed, the mucosa increases in volume: because the ostia are very narrow, it results in the narrowing of their internal lumen until they become occluded. When the ostium of a paranasal sinus is occluded, two very important functions of the latter are altered, namely: stopping the flow of mucus from the paranasal sinuses to the sinus cavities of the nose (thus outward) and, most importantly, preventing the transit of oxygen from the nose to the paranasal sinuses. Stopping the transit of oxygen in the sinuses, in fact, results in the onset of neuropathic pain, or inflammation of the craniofacial nerves.
When an ostium is occluded, the paranasal sinus connected to it takes on the appearance of an air-filled balloon closed at the end. The walls of the paranasal sinus are not impermeable to air as they are lined with ciliated mucosa in which blood vessels are present: these vessels will more or less quickly absorb oxygen trapped in the sinus.
When it has been completely absorbed, a depression forms inside the sinus. This generates a physical force that pulls the mucosa toward the center of the paranasal cavity, as if it were detaching from the bone to which it is anchored. It is the same phenomenon that occurs when air is forcefully expelled from a balloon and its walls tend to collapse against each other.
Rhinosinusitis: pain and infection
Rhinosinusitis: pain and infection
Obviously, the mucosa does not only consist of hair cells, mucipar cells, blood vessels etc. but also of nerve fibers connected to craniofacial nerves. Therefore, when there is the establishment of depression i.e., negative pressure from the outside to the inside, there is a mechanical stress on the nerve fibers that is transmitted and reflected on the craniofacial nerves and from which pain originates.
Moreover, if the situation of complete obstruction of the ostium remains unchanged, as soon as the trapped oxygen is completely depleted, a new process intended to increase pain: the mucosa lining the sinuses will begin to produce a large amount of mucus that evidently cannot exit the affected sinus due to obstruction of the ostium. The mucus itself, then, will eventually exert positive pressure against the mucosa lining the breast (i.e., outward), putting more stress on the nerve fibers and accentuating the pain.
Although what has been highlighted so far summarizes a disastrous situation at the clinical level, the trouble is not over yet: should the situation of the obstruction of the ostium continue much longer, the mucus that has accumulated in the affected sinus, will become infected due to certain pathogenic bacteria that manage in various ways to enter the same sinus. The pain will be overlaid with infection and thus the need to take large amounts of antibiotics.
Why does rhinosinusitis become chronic?
First, there is a distinction to be made based on the type of rhinosinusitis:
- Infectious rhinosinusitis becomes chronic when infected mucus accumulates within one or more sinuses for a long time that fails to be evacuated, and from this inflammation arises that continues over time
- Allergic rhinosinusitis becomes chronic when we remain exposed to an allergenic substance or agent for a long time and is not treated with appropriate medication
- Non-allergic cell-mediated rhinosinusitis (NARES, NARNE, NARMA AND NARESMA) becomes chronic when this is not diagnosed and treated in a timely manner with appropriate and specific drugs (at present there are no highly specific pharmaceuticals for this condition)
In any case, whatever the type of rhinosinusitis, the factors that lead to chronicity of the condition can be summarized as follows:
- Edema (enlargement) of the rhino-sinus mucosa resulting from protracted inflammation
- Slowdown or even arrest of ciliary cell mobility and motility
- Accumulation of mucus-pus in the rhino-sinus area and in the auditory tubes.
What to do in case of rhinosinusitis?
Treating rhinosinusitis is by no means a simple matter for two essential reasons:
- it is necessary to make a precise diagnosis of the etiology of rhinosinusitis i.e. to determine exactly the factor or factors that caused it
- depending on the diagnosed etiology and the stage of the pathology, determine the most appropriate therapy to be practiced
Of course, in order to have an accurate diagnosis, it is necessary to consult an ENT specialist and if necessary, consult the allergist, pulmonologist, and possibly the cytologist.
In the case of rhinosinusitis in children, it is advisable to consult the pediatrician first and then possibly the medical specialists mentioned above, provided that the latter are familiar with children, given their fragile relationship with the physician in general.
However, today it is possible to perform a test to obtain an indication of the possible diagnosis of rhinosinusitis through the development of a diagnostic algorithm developed by our researchers, aimed exclusively at identifying the most suitable Nevia Biotech product to effectively treat the diagnostic pathology through the evaluation of symptoms.



How to effectively treat Sinusitis
There are many drugs on the market used to treat rhinosinusitis, which almost always act only on symptoms, except for antibiotics that act on bacterial infections but are not effective against viral infections (which account for 85 percent of the etiological agents responsible for rhinosinusitis) and fungal infections.
A specific product for the treatment of rhinosinusitis should act simultaneously on the three clinical characterizations of the same rhinopathies, namely: edema of the naso-sinus mucosa, slowing or even stopping of ciliary mobility and motility, and accumulation of muco-purulent secretions in the naso-sinus district and auditory tubes.
Ciliacell is the only product specifically designed to effectively treat rhinosinusitis characterized by the above clinical manifestations, namely, edema of the naso-sinus mucosa, slowing or stopping of ciliary mobility and motility, and accumulation of muco-purulent secretions in the naso-sinus district and auditory tubes.
Ciliacell is a patent-protected product of Nevia Biotech and has been tested in several internationally prominent clinical trials.
The demonstrated clinical healing efficacy is more than 90%.
Nevia Biotech’s Best Products
Choose your option

Recurrent Respiratory Infections

